Introduction
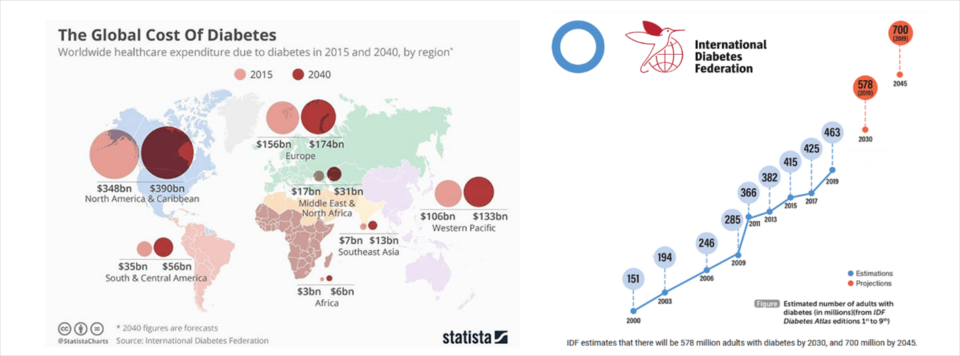
According to the International Diabetes Federation, “over 463 million adults were living with diabetes in 2019, with Type 2 diabetes accounting for around 90% of all diabetes cases.” The estimated healthcare costs exceeded USD 760 Billion.
Type 2 diabetes used to be a ‘mature onset’ disease, but not anymore. As of June 2012, approximately 2,200 ten to twenty-four-year-old Australians were diagnosed with the preventable lifestyle-related disease. Concerningly, the Australian Institute of Health and Welfare (AIHW) suggested around 400 cases of type 2 diabetes are diagnosed each year in those aged 10 to 24 years. Young people are now at risk of developing debilitating comorbidity and diabetes-related complications with premature mortality.
Not since Thalidomide have doctors unintentionally prescribed harm of this scale. Thalidomide use in the late 50s and early 60s caused some 12,000 children worldwide to be born with significant birth deformities.
How many tragic deformities is the current pharmaceutical management of Type 2 diabetes accountable for? Prescriptions based on diabetes guidelines have been shaped by pharmaceutical companies globally.

When will young people lose their eyesight, end up on kidney dialysis, suffer from cardiovascular disease, and the risk of stroke? When will they begin the never-ending debridement of rotting flesh from foot ulcers that will not heal and eventually lead to amputation?

As the incidence of Type 2 diabetes continues to escalate with the force of an approaching tsunami, it is imperative to find lifestyle interventions to protect those in its path.
This issue deserves a 'Bill of Rights'… People deserve to know that Type 2 diabetes is preventable and even reversible and its subsequent life-threatening complications can be avoided.
After decades of simply band-aiding sick-care, believing Type 2 diabetes to be a chronic progressive disease, imagine the joy of empowering people to take back control of their health using 'food as medicine'?
How disappointing, then, to find the American College of Lifestyle Medicine (ACLM) has published this much-needed 'Diabetes Bill of Rights' (Nov 10, 2020) with supporting resources and educational material as an exclusive document rather than an inclusive one.

The authors and facilitators involved in the American College of Lifestyle Medicine (ACLM) position paper (June 8, 2020); their Diabetes ‘Bill of Rights’ (Nov 10, 2020); and their accompanying online course for health professionals (Sept 16, 2020); have deep personal bias and/or devout religious beliefs on diet and nutrition.
While praising the health benefits of cereals, grains, nuts, and soy, they simultaneously cast strong doubts on meat-eating, suggesting it is the cause of Type 2 diabetes, cardiovascular disease, and even cancer. Therefore, it is virtually impossible for the American College of Lifestyle Medicine (ACLM) to consider the health benefits of a low carbohydrate diet, let alone a low carbohydrate diet that includes animal protein and fats, as an option in reversing Type 2 diabetes.
Fully informed about all treatment options?
As stated, The President and Board of Directors of the American College of Lifestyle Medicine do hereby declare the following: - TYPE 2 DIABETES BILL OF RIGHTS
*You have the right to be fully informed about all treatment options for Type 2 diabetes before consenting to treatment. (My edit - The personal bias against animal protein/fats and Low Carb Healthy Fat/KETO principles by the authors of the Position Statement and the Board of Directors of ACLM denies a well-rounded discussion of all treatment options.)
*You have the right to be given accurate, complete, and unbiased information about Type 2 diabetes, pre-diabetes, and insulin resistance, including the benefits of treatment with predominantly whole food, plant-based diet, and other Lifestyle Medicine interventions. (My edit - Again, the personal bias against animal protein/fats and Low Carb Healthy Fat/KETO principles by the facilitators of the 20-module online course for health professionals denies a well-rounded discussion of all treatment options.)
Where is the acknowledgment that an Ancestral Diet, which includes animal protein and fats, is a safe option for managing Type 2 diabetes? The demonisation of animal protein and fats is an undeclared bias.
Concerningly, the authors are either ethical vegans or adherents of the Biblical 'Garden of Eden' diet in keeping with the teachings of the Seventh-day Adventist Church.
The Seventh-day Adventist Health Reform Message
It’s hard to imagine such powerful anti-meat messaging is being accepted as ‘the Gospel truth’ promoted by a Religious group incorporated only 159 years ago. Ellen G White, a founder of the Seventh-day Adventist Church, is considered their Prophetess of Health. She claimed to have experienced over 2000 visions and dreams from God during her lifetime, with the first one occurring at the age of 17. Her Health Reform visions from 1863, have promoted the Biblical Garden of Eden diet - fruits, grains, nuts, and seeds - as the God Appointed diet for man.
This teaching disregards ancestral diets that include animal proteins, fats, and evolutionary hunter-gathering.
Ellen G White claimed God told her that meat was a stimulant, as harmful if not worse, than tobacco, alcohol, and caffeine. Flesh meat aroused baser passions in men, women, and children leading to the heinous sin of ‘Self-Vice’… the puritan term for onanism or masturbation. Masturbation, she taught, defiled people morally, spiritually, and physically.
Among those who are waiting for the coming of the Lord, meat-eating will eventually be done away; flesh will cease to form a part of their diet... We should ever keep this end in view and endeavor to work steadily toward it. I cannot think that in the practice of flesh-eating, we are in harmony with the light which God has been pleased to give us."
Ellen G White taught that it was the duty of “God’s Chosen ‘remnant’ Church”; “His Commandment-keeping people” to warn others of the physical dangers of eating flesh meat and violating the Laws of Nature, authored by God himself.
God gave the light on health reform and those who reject it, reject God
Her teachings continue to influence the advocacy of a plant-based, vegan diet as acknowledged in the publication; - "The Global Influence of the Seventh-Day Adventist Church on Diet" co-authored by Seventh-day Adventist Joan Sabaté MD, MPH, a founding member of the American College of Lifestyle Medicine and a member of the 2020 US Dietary Guidelines committee determining the caps on saturated fat.
ACLM’s TYPE 2 DIABETES BILL OF RIGHTS
The very first statement; - "You have the right to be fully informed about all treatment options for type 2 diabetes," raises questions from the outset.
A 'Bill of Rights' can only be achieved if transparency about the 'plant-biased' messaging promoted by the Seventh-day Adventist Church, which underpins the American College of Lifestyle Medicine's mission.
An inclusive 'Bill of Rights' and supporting dietary toolkit MUST include options for cultural diversity based on where people live and the fresh food they can access locally and seasonally. It cannot be vegan-promoting resources and educational materials shaped exclusively by Religious Ideology and animal rights advocates. The recommendations must be broad and transparent, highlighting minimally processed foods that provide essential protein and fats and essential vitamins and minerals from plants and animals to ensure the best health outcomes for everyone, regardless of personal and religious beliefs.
There is no 'one-size-fits-all.'
Unfortunately, claiming the American College of Lifestyle Medicine's 'Diabetes Bill of Rights' is 'accurate, complete and unbiased' is untrue…
The following discussion requires a balanced perspective to determine the inaccuracies and bias of the American College of Lifestyle Medicine's high carbohydrate, vegan dietary recommendations. Therefore, it is essential to recognise the success of Low Carbohydrate diets in the management of Type 1 and Type 2 diabetes, which has not only been downplayed, ignored, and criticised but even dismissed by the authors and facilitators of ACLM's 'Bill of Rights' and its supporting resources.
An inclusive document looks beyond personal beliefs to offer 'complete and unbiased' information and help empower all people to take back control of their health.
Medical Ethics
Why should an authoritative, well-orchestrated, rallying cry to adopt a vegan diet violate medical ethics?
Two reasons come to mind;
- Firstly - A perceived ‘conflict of interest’ regarding the demonisation of animal protein and fats based on religious ideology.
- Secondly - The Creationist ‘Garden of Eden’ dietary beliefs of the Seventh-day Adventist Church are being pushed onto an unsuspecting public as ‘the Gospel truth,’ denying human evolutionary nutrition and creating the need for lifelong supplementation.
According to the Australian Medical Association (AMA), “the doctor-patient relationship is a partnership based on mutual respect, collaboration, and trust. Within the partnership, both the doctor and the patient have rights as well as responsibilities.” “While they are entitled to have their own personal beliefs and values… doctors and clinicians should avoid ‘prescribing’ religious beliefs or activities or imposing religious and spiritual beliefs on patients.”
ACLM’s Type 2 Diabetes Position Statement
The “Type 2 Diabetes Remission and Lifestyle Medicine: A Position Statement from the American College of Lifestyle Medicine” was co-authored by ACLM founder, Seventh-day Adventist John Kelly, MD, MPH, a facilitator of the Adventist Church-owned CHIP program and Gregory Steinke, MD, MPH, also a member of the Seventh-day Adventist Church. Micaela Karlsen, PhD, MSPH was the third author. She serves as the Director of ACLM’s Lifestyle Medicine Economic Research Consortium (LMERC). It is worth mentioning that LMERC was established as a joint venture between the American College of Lifestyle Medicine (ACLM) and Lifestyle Medicine Institute (LMI) – Developer of CHIP. CHIP, also known as the Complete Health Improvement Program, currently sits under the umbrella of the Seventh-day Adventist Church's commercial arm in Australia… the Sanitarium Health Food Company.
Ellen G White came to Australia (1889 - 1900) to set up the Church, a publishing house, a hospital, and schooling. She also wanted to reproduce the commercial ‘health food’ model founded by Dr. John Harvey Kellogg at the Seventh-day Adventist-owned Battle Creek Sanitarium in the US. But this time, have the Church own it.
The health food business is to supply the people with food which will take the place of flesh-meat, and also milk and butter
Sanitarium Health and Wellbeing Company, one of 20+ global commercial entities of the Seventh-day Adventist Church, is owned and operated by the Australian Health and Nutrition Association Ltd. As part of the Church’s operations Sanitarium is afforded ‘Charity Status’ and as such, pay no tax on the sales of hundreds of commercially processed 'foods' including Weet-Bix and Up&Go, a liquid breakfast cereal. Nor do they pay tax on income from investments or business entities which come under the Sanitarium umbrella which includes Vitality Works and the Complete Health Improvement Program (CHIP) - a wellness program delivered to Churches, Communities and as Corporate Wellness Programs world-wide.
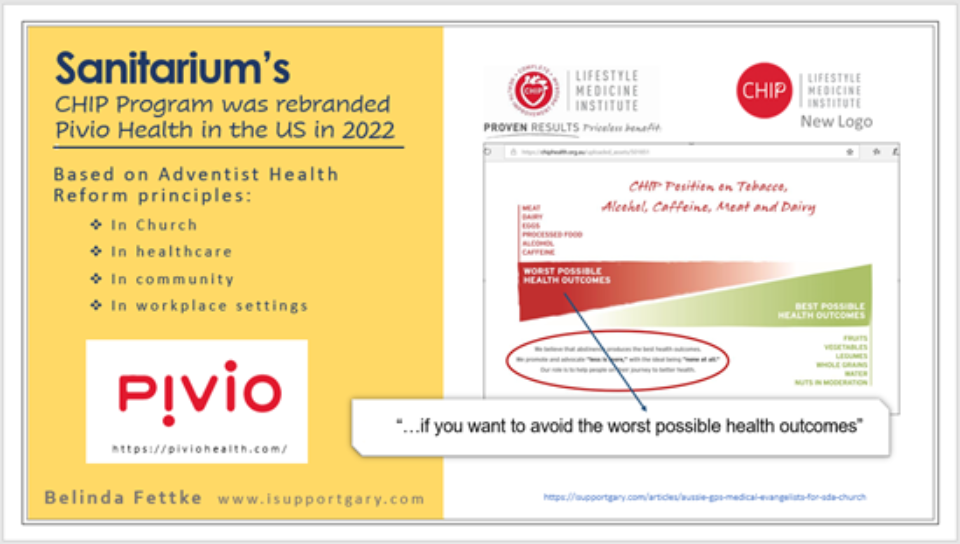
While the Church acknowledges that diet is not a mandate for membership/participation, the following resource from the 2018 CHIP facilitator guide, shows pretty clearly what the Adventist Church's position is on Meat, Dairy and Eggs... They top the list of ‘stimulants’ contributing to the worst possible health outcomes! More dangerous than processed foods and alcohol???
Many of the authors and facilitators involved across ACLM's Type 2 Diabetes remission projects are involved in delivering and promoting the Church's CHIP program.
CHIP has been endorsed by the Physicians' Committee for Responsible Medicine (PCRM), founded by Neal Barnard (an ACLM T2D Facilitator). Up until December 2020, CHIP was also endorsed by the International Nutrition Research Foundation, incorporated in 1989 by Adventist Dr. Hans Diehl at Loma Linda University… Seems he is endorsing the very program he founded!
Incidentally, ACLM's support and promotion of CHIP (originally known as the Coronary Health Improvement Program) goes back to its founding in 2003 when the course was still under the guidance of its creator and the Lifestyle Medicine Institute was based at Loma Linda University.
CHIP was officially endorsed by the American College of Lifestyle Medicine in 2020.
As of Feb 2022, Sanitarium’s CHIP program was relaunched in the US as Pivio Health and again endorsed as per the screen grab below. It acknowledges (Adventist) Dexter Shurney MD as the author congratulating Pivio. He has been instrumental in getting the CHIP program up and going at Vanderbilt University and at Cummins Inc when he was employed there.
The authors declared “no conflicts of interest with respect to the research, authorship, and/or publication” of ‘Type 2 Diabetes Remission and Lifestyle Medicine: A Position Statement from the American College of Lifestyle Medicine’ despite it being supported financially by the American College of Lifestyle Medicine… an organisation John Kelly MD founded in 2003 on the Seventh-day Adventist Church’s Loma Linda University Campus, California, as the Christian Association of Lifestyle Medicine.
It is essential to note the authors' conclusion from their Position Statement was; that "to achieve remission, appropriate, therapeutic dosing of lifestyle modifications is necessary, including a hypocaloric diet." They continue; - "Future research should focus on high-quality intervention trials… including consumption of a low-fat, WFPB diet to achieve remission of T2D in comparison to standard pharmacologic treatment and surgical interventions.”
Unfortunately, ACLM's conclusion does not suggest intervention trials comparing 'Low Fat' to 'Low Carb/Keto' diets despite impressive results published here, here, here, and here… without calorie restriction..
ACLM’s latest resources depict their version of a ‘Whole Food Plant-Based’ (WFPB) diet – completely devoid of animal protein or dairy, even for children.
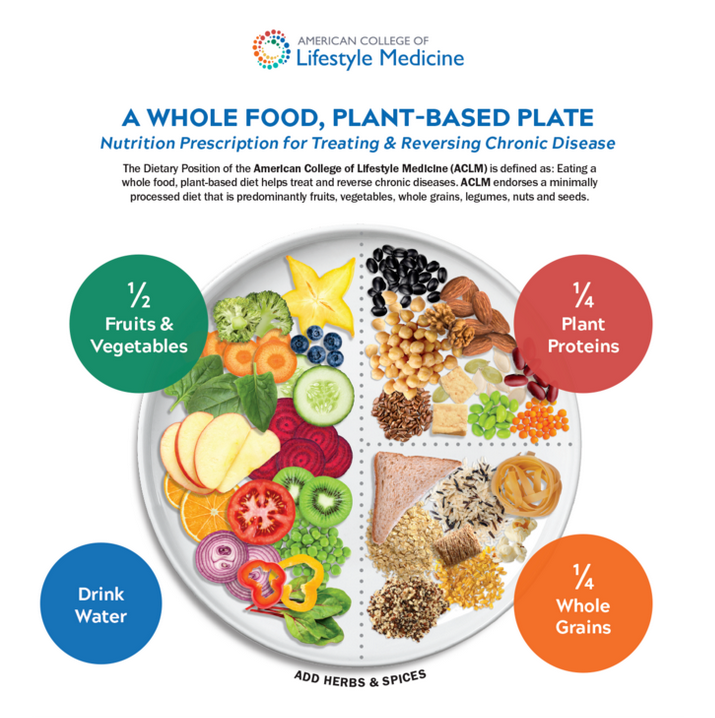
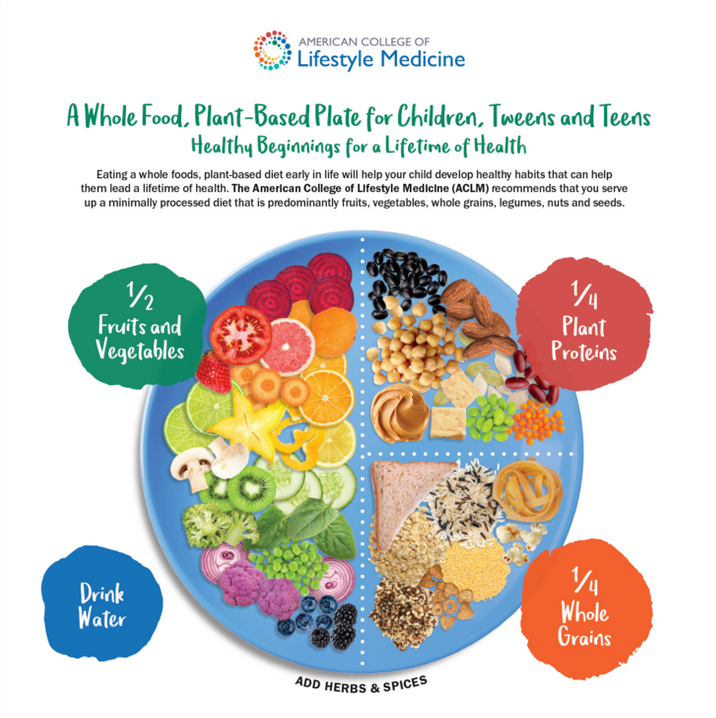
I understand this is their belief. But, where is the transparency for those who do not ascribe to the dietary teachings of the Seventh-day Adventist Church?
Delving into the references used to discredit Low Carbohydrate Diets
Type 2 Diabetes Remission and Lifestyle Medicine: A Position Statement From the American College of Lifestyle Medicine
John Kelly, MD, MPH, Micaela Karlsen, PhD, MSPH, Gregory Steinke, MD, MPH
https://doi.org/10.1177/1559827620930962
Article first published online: June 8, 2020; Issue published: July 1, 2020
The screen-grab below highlights the ACLM author’s cherry-picked excerpts from studies to create the illusion of it aligning with their beliefs, suggesting a low carbohydrate diet is not a 'healthy' or safe option in the reversal of Type 2 diabetes. Incredibly, the conclusions of the majority of the references do not support the 'bite-sized' claims outlined in the ACLM article.
I have transcribed the above text, including the references quoted, plus an earlier section of the article sharing the history of managing diabetes, to highlight the research used in the dismissal of the role of Low Carbohydrate diets in the management of Type 2 diabetes and to challenge the authors' conclusions.
The Historical Context
Although the concept of using diet to achieve remission seems new in the context of conventional treatment, it is not a new idea. Over the course of the 20th century, diet recommendations for diabetes prevention and management varied widely,59 alternately supporting either low-carbohydrate/high-protein60,61 or high-carbohydrate62-65 eating patterns. However, instead of remission as a goal, research typically focused on glycemic improvement and disease management.8,66,67
During that time, the use of medication emerged as the primary means of treatment.8 The discovery of insulin in 1921 was hailed as a breakthrough therapy for severe diabetes,68 later known as type 1 diabetes. While this discovery of insulin was life-saving for patients with type 1 diabetes, it also became the standard of care for patients with type 2 diabetes.
References 60 and 61 appear to have been 'ignored in the Low Carbohydrate section' altogether… instead, lying obscured in the 'history section' where they sit without acknowledging their positive results.
Reference 60 was published in October 2018, not before the invention of insulin, as the context positioning within the ACLM article infers.
- Findings: - "The ketogenic diet substantially reduces the glycemic response that results from dietary carbohydrate as well as improves the underlying insulin resistance. This review combines a literature search of the published science and practical guidance based on clinical experience."
- "While the current treatment of T2DM emphasizes drug treatment and a higher carbohydrate diet, the ketogenic diet is an effective alternative that relies less on medication and may even be a preferable option when medications are not available."
- Plasma lipids reverted to normal in half of these patients after dietary treatment for one month… Specialized and complex diets or lipid-lowering drugs are unnecessary in the majority of patients."
Reference 61 "The effect of dietary carbohydrate restriction on lipid abnormalities has been examined in 42 newly diagnosed maturity-onset diabetics…"
I have to ask, "Were these two studies omitted from the 'Low Carbohydrate' discussion because they didn't fit ACLM's cherry-picked narrative?"
What else do they say?
Remission requires an energy deficit to remove liver and pancreatic triacylglycerols and stop their lipotoxic effects. Thus, consuming low GI foods alone cannot produce remission without an energy deficit. Some low GI dietary patterns that help maintain a low SG do not reverse insulin resistance and do not produce T2D remission. One such pattern is the so-called “ketogenic diet,” which emphasizes a low-carbohydrate, high-fat, and high-protein eating pattern.78
A VLED produces ketosis, but does it with an energy deficit, whereas the ketogenic diet does it by forcing the body to metabolize fats instead of carbohydrates. The diet is not energy deficient and does not reverse liver and pancreatic triacylglycerols; thus, it helps control SG but not insulin resistance.78 79 Ketogenic diets only appear to eliminate T2D by consistently failing to challenge insulin receptivity rather than by improving or restoring it.
Low-Carbohydrate Diets
The present swing toward a high-protein, low-carbohydrate dietary pattern for improving hyperglycemia is problematic. As summarized by Uusitupa and Schwab in their editorial on diet and T2D,80
. . . there are no real long-term intervention trials on high protein diets in people with diabetes.81 . . . the safety of high protein diets has been documented for one year only.81 . . . the quality or quantity of dietary protein does not seem to play any role in the pathogenesis of type 1 diabetes, whereas regarding type 2 diabetes, higher intakes of red meat and processed meat products have been consistently associated with the increased risk of type 2 diabetes82 and other chronic non-communicable diseases.83 This should arouse concern when considering any dietary guidelines.
Long-term prevention trials of T2D have applied diets emphasizing healthy dietary patterns with typical protein intake.84 The primary goal of the prevention of T2D is permanent weight reduction that can be achieved by healthy dietary patterns and increased physical activity.
“The diet is not energy deficient and does not reverse liver and pancreatic triacylglycerols; thus, it helps control SG but not insulin resistance.” ... only if you’re a mouse!
- Dr. Andreas Eenfeldt, MD explains; - “In the study, researchers fed mice (!) a keto diet for three days (!), and then ran a glucose tolerance test. They noticed that while the mice on a keto diet had a lower fasting blood glucose, it got higher after the glucose tolerance test and there were signs of a reduced effect of insulin compared to mice on regular mouse chow. That’s basically it.”
- Most importantly, Dr. Eenfeldt concludes; - “a number of long-term studies (over months and years) and decades of experience in actual humans show that a keto diet reverses type 2 diabetes.”
“Adding more fat to a high-fat diet only exacerbates hepatic insulin resistance”… if you’re a mouse!
- This Journal Club article simply rehashes the findings from Reference 78. That’s all it does… repeat/reward?
“The present swing toward a high-protein, low-carbohydrate dietary pattern for improving hyperglycemia is problematic. As summarized by Uusitupa and Schwab in their editorial on diet and T2D”
- “So far, no long-term prevention studies with a high protein diet exist.”
- “One argument not to recommend high protein diets in the longer-term is that this kind of a diet may cause concern when adjusting dietary patterns to a lower protein intake when necessary, e.g., regarding the development of renal diseases” (This is a serious quote from the article!)
- “Furthermore, in the future, ecologic issues should be considered with regard to dietary recommendations.”
The cherry-picked comment about; - "no real long-term intervention trials on high protein diets in people with diabetes" and "the safety of high protein diets has been documented for one year only" barely explain the context of the article…
Before discussing what may or may not be ‘safe’ it is worth mentioning that the Conflict-of-interest statement accompanying this article is… illuminating.
- "Patients with a GFR <60 mL/min/1.73 m2 did not show a faster decline of GFR or kidney function with protein intakes around 0.8 g/kg body weight as compared with lower intakes, thereby arguing against a (protein) restriction."
- “We concluded that no association is observed between protein intake and mortality in observational studies in people with diabetes. (quality of evidence: very low).”
- "The effects of protein intake on diabetic eye or nerve disease have not been reported."
- "There are a number of studies that have compared different types of animal proteins (milk, chicken, beef, pork, and fish) or compared animal with plant protein in diabetic patients and have reported a greater reduction of serum cholesterol with plant protein."
But, who wants to lower serum cholesterol?
Zoë Harcombe Ph.D. explains why cholesterol is essential
"If you had no cholesterol in your body, you would have no cells, no bone structure, no muscles, no sex hormones, no reproductive system, no digestion, no brain function, no memory, no nerve endings, no movement... no human life."
The study findings continue.
- "We concluded that higher protein weight-loss diets caused a significantly greater reduction of systolic and diastolic blood pressure than lower protein diets in people with T2D.”
- "A primary problem of most studies is the poor compliance of study subjects with the recommendation of lower protein intake."
- "In summary, the suggested range of protein intake appears to be safe and can be adapted according to personal dietary preferences."
“higher intakes of red meat and processed meat products have been consistently associated with the increased risk of type 2 diabetes.”
Consistently associated? The quote from the ACLM authors appears to be not only an exaggeration but not synonymous with the findings of the systemic review; -
- “Overall, the association between dietary factors and type 2 diabetes has been extensively studied, but few of the associations were graded as high quality of evidence.
- “These findings could be of importance for the prevention of the disease. However, the strength, precision, and influence of potential bias regarding these associations need to be clarified.”
There are three obvious flaws of epidemiology: association not causation; relative not absolute risk; and the healthy person confounder...
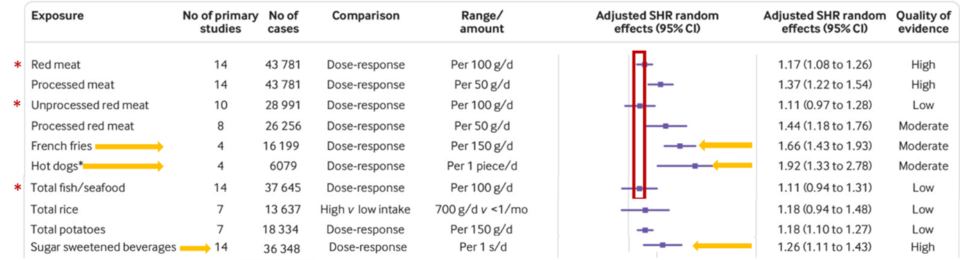
Ignoring the fact that this review of meta-analyses relies on food frequency questionnaires, diet history, and 24-hour dietary recalls, which come with their own inherent flaws, the collated table clearly demonstrates the “evidence of associations” between ‘red meat’, ‘unprocessed red meat’, and ‘fish/seafood’ with the incidence of type 2 diabetes, are very similar. Which begs the question as to why red meat has become so vilified? If anything, people should be warned about hot dogs (especially the white bun and the sauces), French fries (doused in polyunsaturated seed oils) and coke!! A highly processed recipe for disaster…

The series of systematic reviews and meta-analyses in this study do not support the claims of “higher intakes of red meat and processed meat products have been consistently associated with the increased risk of other chronic non-communicable diseases.”
In fact, red meat is not even mentioned in this article! It is about fibre…
- "This coming together of the epidemiological and experimental work on fibre allows conclusions to be drawn that increased fibre intakes should result in improvements in population health."
- NOTE: - "Our findings are limited to risk reduction in the population at large rather than those with chronic disease."
How can the authors then claim; - “This should arouse concern when considering any dietary guidelines.”
“Long-term prevention trials of T2D have applied diets emphasizing healthy dietary patterns with typical protein intake.”
Before discussing what may or may not be ‘healthy dietary patterns’ it is worth mentioning that the Conflict-of-interest statement accompanying this article is once again… illuminating.
The authors concluded; -
- "We have a high certainty of evidence that T2D is preventable by changing lifestyle, i.e., weight reduction by diet change according to the current recommendations in terms of quality of fat, fiber intake, increased use of whole-grain products, fruit, and vegetables, and increasing physical activity.
- "Additional well-controlled intervention studies are needed to identify the optimal diet to prevent T2D."
Sarah Hallberg MD shared a graphic of the carbohydrate intake of all the studies claiming that a Low Carbohydrate diet is associated with increased mortality.
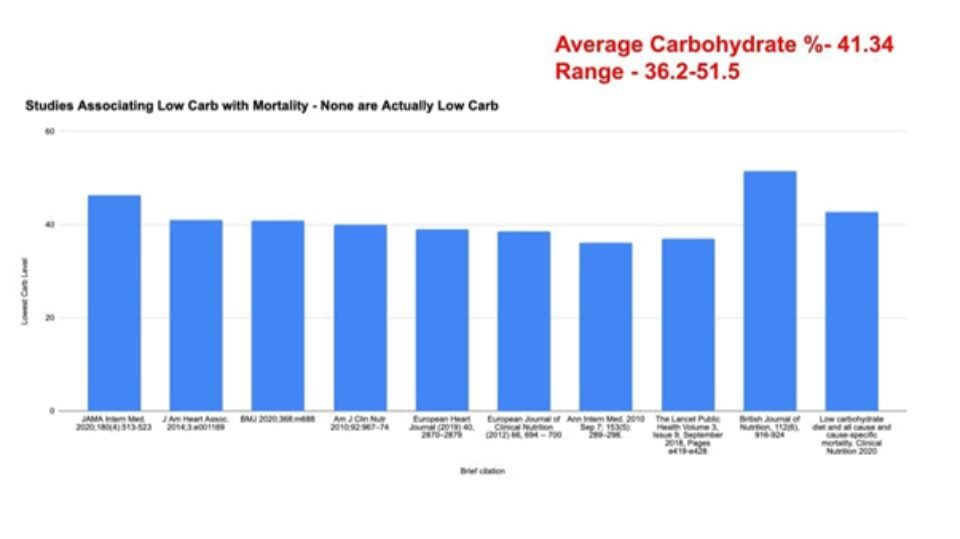
With an average of 41.34% as a daily intake of carbs, none were even close to the recommended Therapeutic Carbohydrate Restriction of a Low Carb or Ketogenic diet and, in fact, far closer to the Standard American Diet, frequently referred to as 'SAD.'
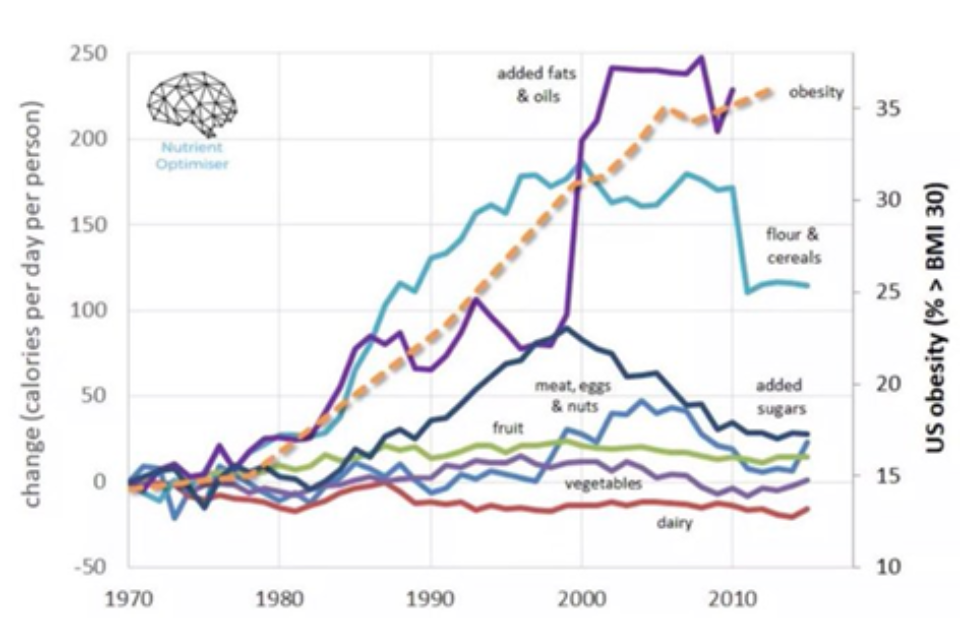
Blaming meat, eggs, and dairy for the tsunami of obesity and Type 2 diabetes does not make sense. Despite a more recent decline in flour and cereals, depicted in the graphic below, their caloric intake has been high since the introduction of the worldwide dietary guidelines. According to data collected at Optimising Nutrition, "the big change in caloric intake is from added fats and oils extracted from soy, corn, and rapeseed, has literally been poured into our food system," coincides with an explosion of obesity and metabolic disease, most notably Type 2 diabetes.
While I wholeheartedly agree with ACLM's position that "Diabetes reversal should be (the) goal in managing Type 2 diabetes,"… The Counterpoint study referenced above is a calorie-restricted program where people are required to use commercially produced ‘soups and shakes’ to lose weight. Concerningly, several Counterpoint study authors and researchers are financially invested and/or have been found to have ties to Counterpoint and Counterweight programs and products, and/or pharmaceutical companies selling diabetes medications. Professor Mike Lean, co-author of the DiRECT study, not only acknowledges funding from Novo Nordisk, the Cambridge Weight Plan, and Counterweight, but he also owns shares in a company providing pizza toppings and sauces for school lunches!
The Counterpoint and DiRECT studies are referenced on the Cambridge Weight Plan website, which involves the direct selling of ‘soups and shakes’ and highly processed snacks via consultants, including health professionals.
In early 2004 the Christian Association of Lifestyle Medicine (CALM) officially became the American College of Lifestyle Medicine (ACLM). At the time, all nine office bearers and directors were members of the Seventh-day Adventist Church.
The 2004 ACLM website listed resources, for years, that included slide presentations by founder Dr. John Kelly on cardiovascular disease and diabetes management referencing Ellen G White, the Bible, and the Adventist Health Reform message.
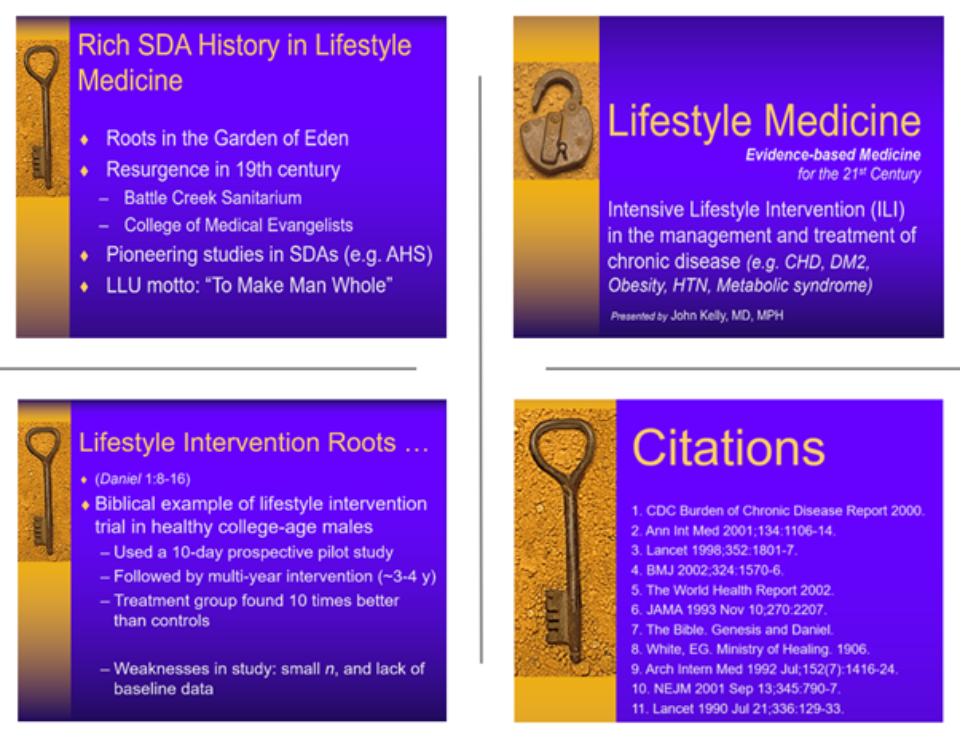
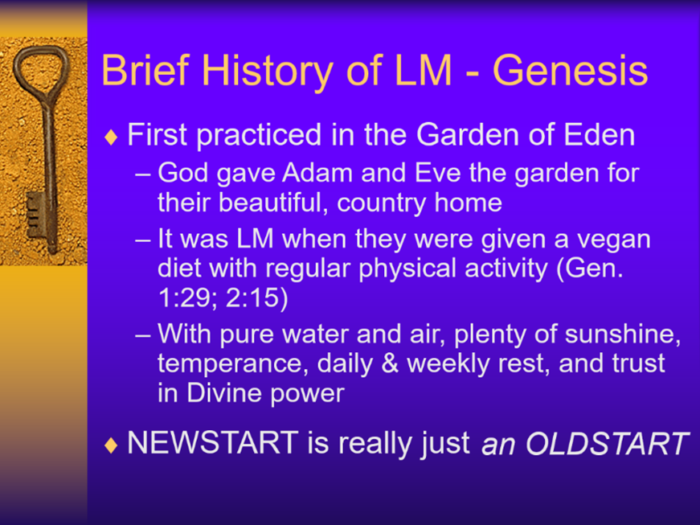
Dr. John Kelly's presentation 'Lifestyle Medicine: evidence-based medicine for the 21st century’ not only outlines a brief history of Lifestyle Medicine in Genesis but claims Lifestyle Medicine was first practiced in the Garden of Eden.
It was Lifestyle Medicine when Adam and Eve were given a vegan diet with regular physical activity, pure water, and air, plenty of sunshine, temperance, daily and weekly rest and trust in divine power
The 'Diabetes Bill of Rights' is a companion piece to the (ACLM) American College of Lifestyle Medicine's "Reversing Type 2 Diabetes and Insulin Resistance with Lifestyle Medicine" - an online course for health professionals.
"Reversing Type 2 Diabetes and Insulin Resistance with Lifestyle Medicine" - an online course for health professionals
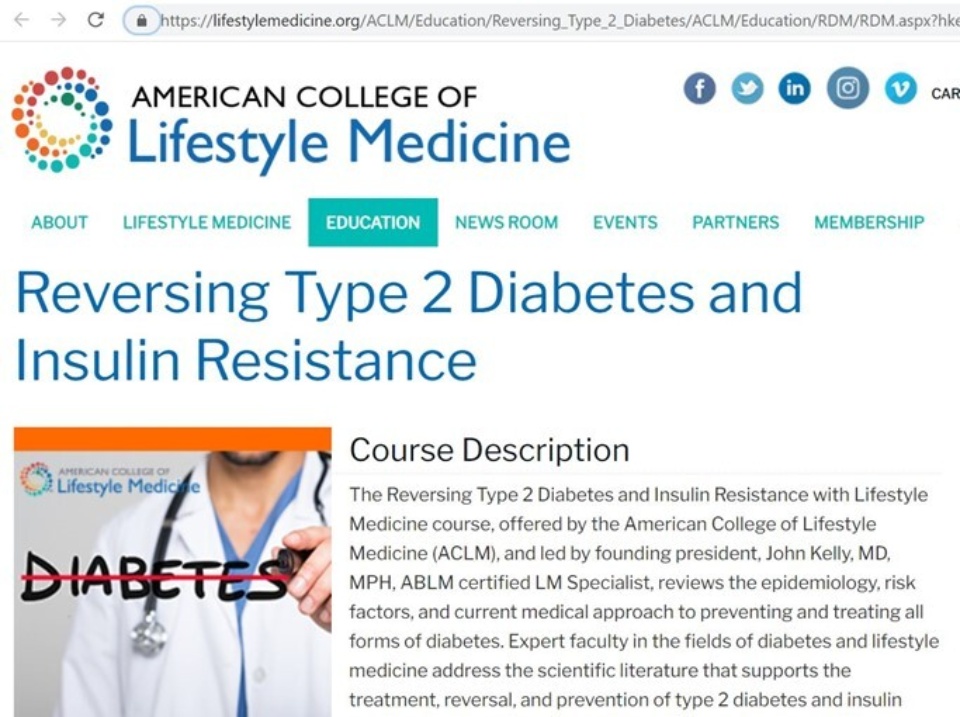
Members of the Seventh-day Adventist Church facilitating modules, and those aligned with the Adventist Health Reform message, are promoting a plant-based diet as the ‘Gospel Truth’ without sufficient transparency as to why they are demonising animal protein and fats.
John Kelly MD
- Founding President of the American College of Lifestyle Medicine in 2003, on the Seventh-day Adventist Church-owned Loma Linda University campus
- A passionate advocate of Lifestyle Medicine
- Co-Author of "Type 2 Diabetes Remission and Lifestyle Medicine: A Position Statement from the American College of Lifestyle Medicine" and the Foundations of Lifestyle Medicine Board Review manual
- CHIP facilitator for community immersion and training of health professionals
Wes Youngberg MD
- Founding director of the American College of Lifestyle Medicine
- Assistant clinical professor at Loma Linda University Schools of Medicine & Public Health.
- Facilitator of the Adventist Canvasback Missions inc; a lifestyle intervention program operated in the Guam Seventh-day Adventist Clinic. A modified version of the NEWSTART® wellness program (a lot like CHIP)
George Guthrie MD
- Founding member and Past President of the American College of Lifestyle Medicine (2016-2018)
- Involved in the development of several Adventist Health programs, including CHIP
- Co-author of ACLM's 2018 anti-animal protein/fat Dietary North Star
Other facilitators include vegan advocates; -
Brenda Davis
- Vegan Dietitian, involved with Dr. John Kelly and Loma Linda University’s 2006 Defeating Diabetes program in the Marshall Islands - based on the Seventh-day Adventist NEWSTART/CHIP program in Guam that Dr. Wes Youngberg was also involved in. It was acknowledged that after 2 weeks the indigenous people (Chammoro) were allowed to reintroduce fish, their most important source of protein, back into the vegan diet prescribed to them... if they chose.
- Incredibly, “Due to a lack of funding after the clinical trial ended, the study data was not analyzed and published until 2019."
Neal Barnard
- Founding president of the Physicians Committee for Responsible Medicine (PCRM) in 1985. PCRM has endorsed the Adventist CHIP program for decades.
- Vocal in his advocacy for a vegan diet and equally vocal in his objections to animal protein, fats, and Low Carb diets

- Conducted an RCT low-fat vegan study and compared it to the conventional diabetes diet to treat Type 2 diabetes. He concluded success as a 0.3% decrease in HbA1c, quoting best results of 0.8%.
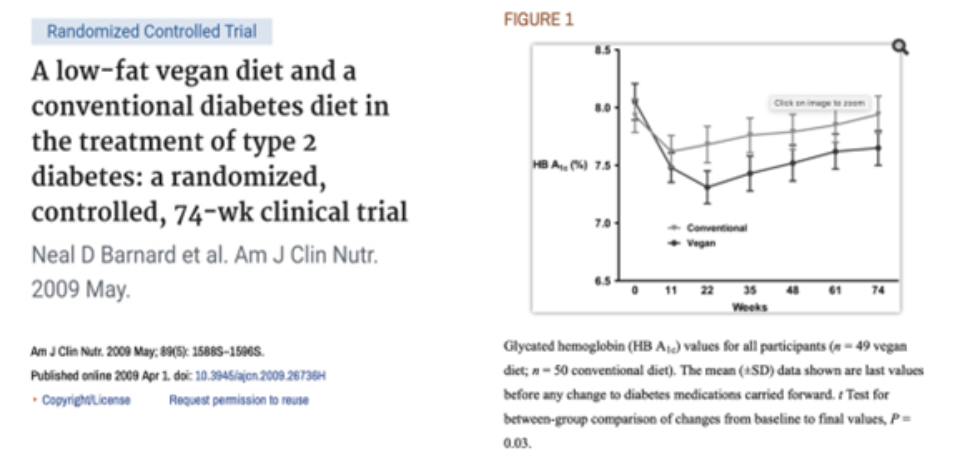
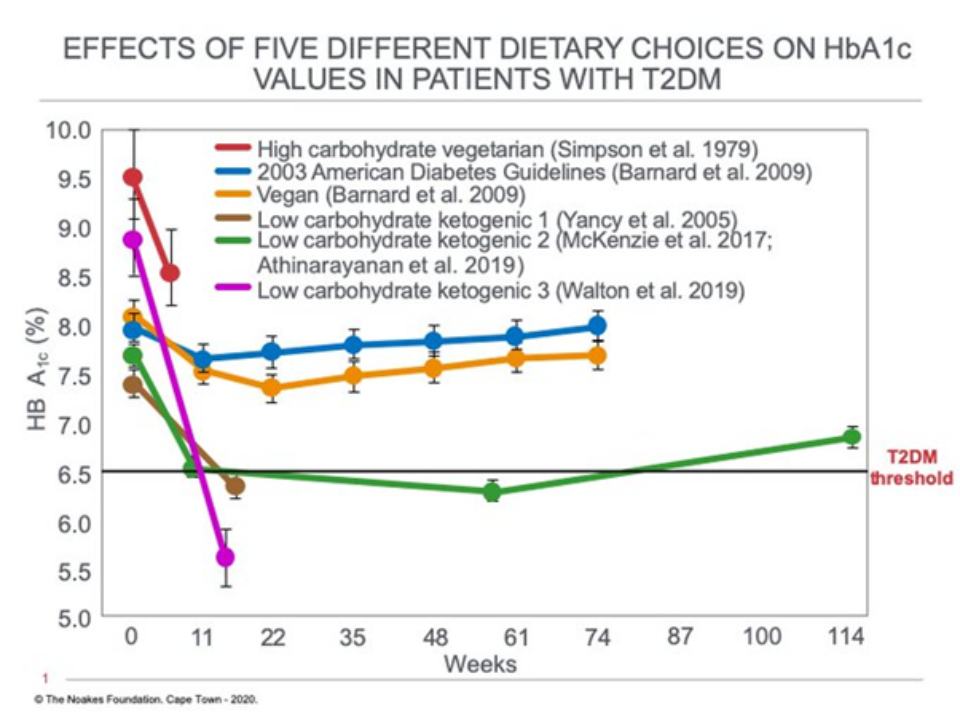
A comparison of Barnard's results to other studies of the ‘effects of dietary interventions on HbA1c’ was shared recently by Professor Tim Noakes, highlighting the effectiveness of Low Carbohydrate/Ketogenic diets for people with Type 2 diabetes, which should be acknowledged.
Cyrus Khambatta
- Has Type 1 diabetes himself and acknowledges trying Low Carb (100-125grams) without success. 100-125g of carbohydrate is not considered an optimal Therapeutic Carbohydrate Restricted 'low'.
- Co-founder of Mastering Diabetes program with Robby Barbaro
Marty Kendall has written an article titled ‘vegan vs keto’ which includes a discussion of the Mastering Diabetes program co-founded by Cyrus, and notes that; -
"Cyrus is highly active and practices intermittent fasting. His Hba1c is in the high 5's. Robbie has a Hb1c in the low 6's. Granted, this is good compared to the majority of the Type 1 population."
"They'll have a better chance of thriving with good blood sugars if they are eating lots of vegetables and fruit compared to more processed grains and sugars that make up the typical diet. But it's still a far cry from the blood sugar control of people following the type of low-carb approach advocated by Dr Richard Bernstein.”
"A significant portion of the Mastering Diabetes video was devoted to explaining their new creative definition of insulin sensitivity. The fundamental problem with this central piece of the Mastering Diabetes argument is that it conflates basal and bolus insulin. Your basal insulin is irrelevant if you are trying to do this sort of insulin sensitivity calculation!
"If you take the denominator to your insulin sensitivity calculations to be the basal + bolus insulin, then the high carb approach has a better insulin sensitivity. If you only consider the bolus insulin (the only sensible approach in my view), then you declare the low-carb approach to be the winner.
*Bolus insulin is taken with food and is proportional to the insulin load of the food they eat (i.e., carbs – fibre + half protein)
*Basal insulin is the insulin that your pancreas would produce throughout the day and night whether or not you eat anything.
"The problem with the argument that normal blood glucose fluctuations are between 70mg/dL to 145 mg/dL or 3.8 to 8.0mmol/L is that what currently passes for 'normal' is far from optimal. Complications from diabetes start to kick in well below what is widely considered 'normal.'"
Marty concludes, "Hence my quest to understand how we can make intelligent food choices to optimise blood sugar and insulin levels. Insulin resistance and metabolic syndrome are a big deal, so let's not ruin more lives than we need to with advice that is based on bad math or putting ethical convictions or religious beliefs ahead of human health."
I wholeheartedly agree.
Dean Sherzai
- Co-director of the Brain Health and Alzheimer's prevention program at Loma Linda University Health.
- He made the comment: - "There is no one-size-fits-all brain diet, although the Mediterranean and MIND diets are good examples of healthy, brain-healthy eating plans." "Whatever you call it, at its core, it's plant-based, i.e., rich in fruits, grains, vegetables, legumes, nuts, and seeds. These foods are rich in antioxidants; they also provide much of the B12, choline, and protein your brain needs to do its job without having to take a supplement." (Ummm, plants provide abundant B12??? That's news to me!)
Vitamin B12
Even the Adventist Health Ministries discuss issues of B12 deficiencies on a 'total vegetarian' (vegan) diet on their website, stating; - "It is important to note that inactive analogs of vitamin B12 may be present in some foods such as spirulina, seaweed, and fermented foods such as tempeh. While food labels may claim the presence of vitamin B12 in these foods, they do not provide any significant level of active vitamin B12 (cobalamin) useful for the body. Small amounts of vitamin B12 are found in white button mushrooms, but they cannot be relied upon as a significant dietary source."
(EDIT) The Adventist Health Ministries removed the original fact sheet in 2022 following their General Conference, but it is still available on the internet archive and downloaded here; Fact Sheet Vitamin B12 For The Vegetarian Adventist Health Ministries 2019.
I am fascinated by the answer to their own question; - "Why is B12 fortification of a plant diet necessary today if the original diet was ideal and ensured optimal health?"… "We don't know. In past centuries, B12-synthesizing intestinal flora may have inhabited the small intestine of humans, making B12 absorption in the ileac region a distinct possibility. Changes in the gut flora of humans over time could have occurred, making B12 production occur lower down in the colon, and hence unavailable for absorption. Also, ideally, natural contamination of foods and water with vitamin B12 could have occurred in the conditions of creation. Furthermore, we are unaware of the nutritional content of the fruit from the tree of life in the Garden of Eden. The tree was removed from access to men and women after the Fall.
But… "We are sure of one thing: Long periods of no B12 intake produce serious clinical signs of B12 deficiency that impair our health." Adventist Health Ministries.
Scott Stoll
- Co-founder of The Plantrician Project, The International Plant-Based Nutrition Healthcare Conference, and The International Journal of Disease Reversal and Prevention
- Instrumental in the founding of Doctors for Nutrition promoting vegan diets in Australia/NZ
- Interviewed with Hans Diehl (Founder of CHIP) on the Adventist 3 Angels Broadcasting Network 2018
Denise C Fields
- CHIP facilitator, and now participates in the training of new CHIP facilitators at the Cummins LiveWell Center. (Founded by past-president of ACLM; Member of the Seventh-day Adventist Church; Elder Dexter Shurney)
Jeni Shull
- Loma Linda University for residencies in family and preventive medicine serving as chief resident for both programs. Multiple committees advocating for Lifestyle Medicine for both patients and colleagues.
- Became the first fellow in the Black Hills Lifestyle Medicine Fellowship under John Kelly MD (founder of ACLM), sponsored by Cummins Inc
- Upon completion of her training, Dr. Shull joined Premise Health, the firm that runs the LiveWell Center for Cummins Inc in Columbus, Indiana using the Adventist Lifestyle Medicine Institute’s CHIP program as a result of past-president of ACLM, Dexter Shurney, MD.
- Co-authored the Foundations of Lifestyle Medicine Board Review manual with Seventh-day Adventist John Kelly MD
“God is the author of science” - Ellen G White
As Young-Earth Creationists, the idea of an Ancestral or Evolutionary diet; one that suggests we have evolved from 'Hunter/Gatherers' and includes animal proteins and fats, is not 'science.'
Gerard Pfandl, a Seventh-day Adventist, makes the point; - "This was not something she (Ellen G White) believed because she took Genesis 1 seriously; she wrote; "I was then carried back to the creation and was shown..." (3SG 90)
"The Bible," she said, "is not to be tested by men's ideas of science… (CT 425) because "nature and the Bible had the same author." Therefore, 'science,' based on the conceptions and theories of men (thereby placing that which has been created above its creator) was for her “stamped with idolatry”.
"One of the greatest evils that attends the quest for knowledge, the investigations of science, is the disposition to exalt human reasoning above its true value and its proper sphere." (MH 427)
Within the Seventh-day Adventist Church, 'Evidence-based medicine' is that which is supported by the Bible. Therefore, the Biblical Garden of Eden diet - 'fruit, nuts and seeds' - IS the God-appointed diet for man. End of discussion.

Is the Seventh-day Adventist Church's Medical Evangelism compatible with Medical Ethics?
It is clear from the 2015 publication by Ruben Sánchez Sábaté et al., Feeding Holy Bodies: A study on the social meanings of a vegetarian diet to Seventh-day Adventist church pioneers” that diet and nutrition became: -
- A way to nourish their new identity with moral and spiritual purity
- A demonstration of their commitment to the Adventist message
- A medium to communicate values and ideas
- A tool to open doors to evangelise
- A way to take the gospel to the people
In a recent submission to the Australian government, the Seventh-day Adventist Church wrote; - "We do not wish to compel or force any person to act or believe in a certain way, however, in return, we request that we as believers… have the freedom to be able to provide services and ministries to people who are attracted to the biblical beliefs, tenets, teachings, and doctrines espoused." (My emphasis)
Medical Evangelism is the Right Arm of the Church and their ‘Health Reform Message’ is to be used as the ‘Entering Wedge’.
Manuscripts. 58, 1901, Evangelism 513:1 (Ellen Gould White)
“Nothing will open doors for the truth like evangelistic medical missionary work. This will find access to hearts and minds and will be a means of converting many to the truth.”
According to the Australian Medical Association (AMA), "the doctor-patient relationship is a partnership based on mutual respect, collaboration, and trust. Within the partnership, both the doctor and the patient have rights as well as responsibilities." "While they are entitled to have their own personal beliefs and values… doctors and clinicians should avoid ‘prescribing’ religious beliefs or activities or imposing religious and spiritual beliefs on patients.”
To have “the freedom to be able to provide services and ministries to people who are attracted to the biblical beliefs, tenets, teachings, and doctrines espoused" as stated by the Church, would require complete transparency around the plant-biased messaging promoted by the Church and its members. Plant-biased messaging with far-reaching effects on medical and dietetic education, our dietary guidelines, and food labeling.
Inclusive Type 2 Diabetes Reversal/Remission
There are currently three accepted ways to put Type 2 diabetes into reversal or remission (ACLM uses both terms), recognising the likelihood of achieving this goal is greater in patients with a shorter duration of the disease and those not already taking insulin.
- Bariatric surgery involves operating on a healthy organ for a dietary disease.
- Very Low-Calorie Diet (VLCD), also known as a Very Low Energy Diet (VLED), where commercially processed 'soups and shakes' are used as meal replacements (Lean 2017, Taylor 2018, Lean 2019)
- Low Carbohydrate/ Ketogenic Diets (Hallberg 2018, Athinarayanan 2019, Unwin) using Therapeutic Carbohydrate Restriction guidelines (Adele Hite LowCarbUSA)
The terms Reversal where an HbA1c <6.5% is achieved without diabetes medications (but may include Metformin) and Remission, defined as HbA1c <6.5% achieved without any diabetes medications and maintained for at least one year, describe the regression of hyperglycaemia and insulin sensitivity to pre-diabetes levels.
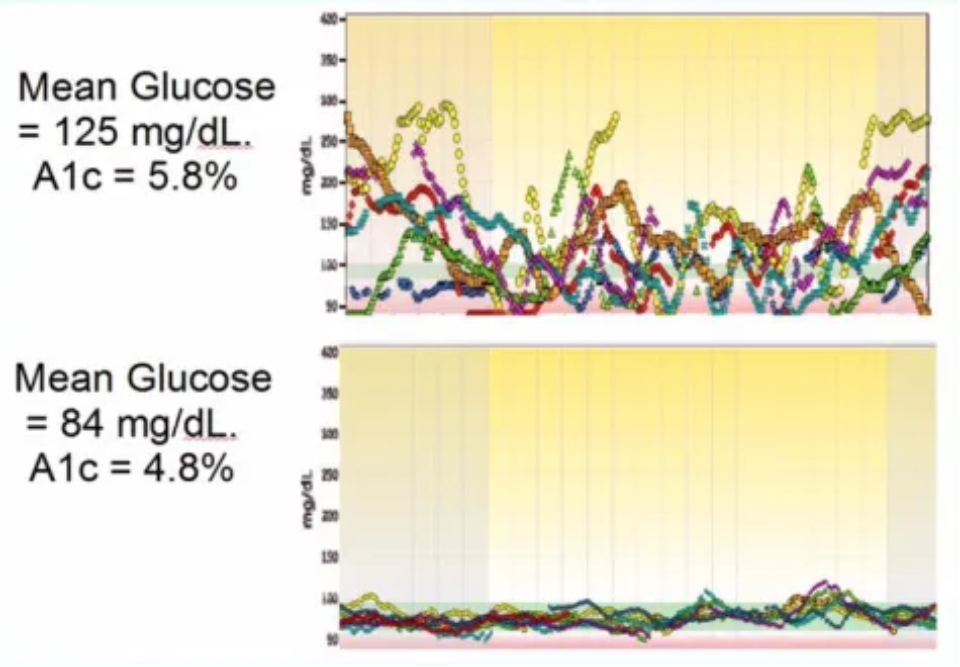
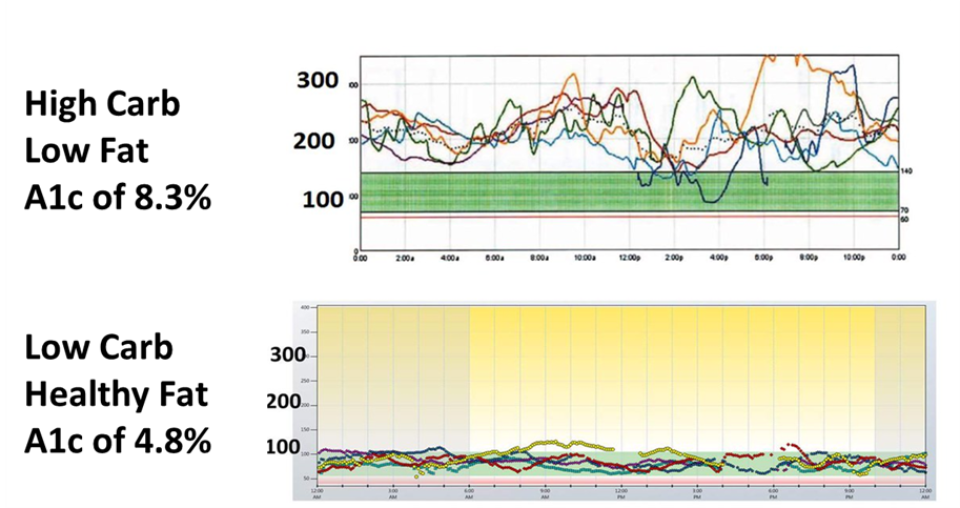
Imagine if the goal was normal blood glucose with minimal fluctuations? Where the HbA1c is equal to or <5.6%?
Therapeutic Carbohydrate Restriction
Dr. Russell M. Wilder understood from 1916 that diabetes was a disease of carbohydrate intolerance and used a ketogenic diet in the clinical management of diabetes even before its use in the treatment of Epilepsy. Wilder’s protocol for individualising Therapeutic Carbohydrate Restriction below 60g, combined with Intermittent Fasting, enabled patients at the Mayo Clinic (before the invention of insulin) to control their blood glucose, as outlined in the book A Primer for Diabetic Patients (1922).
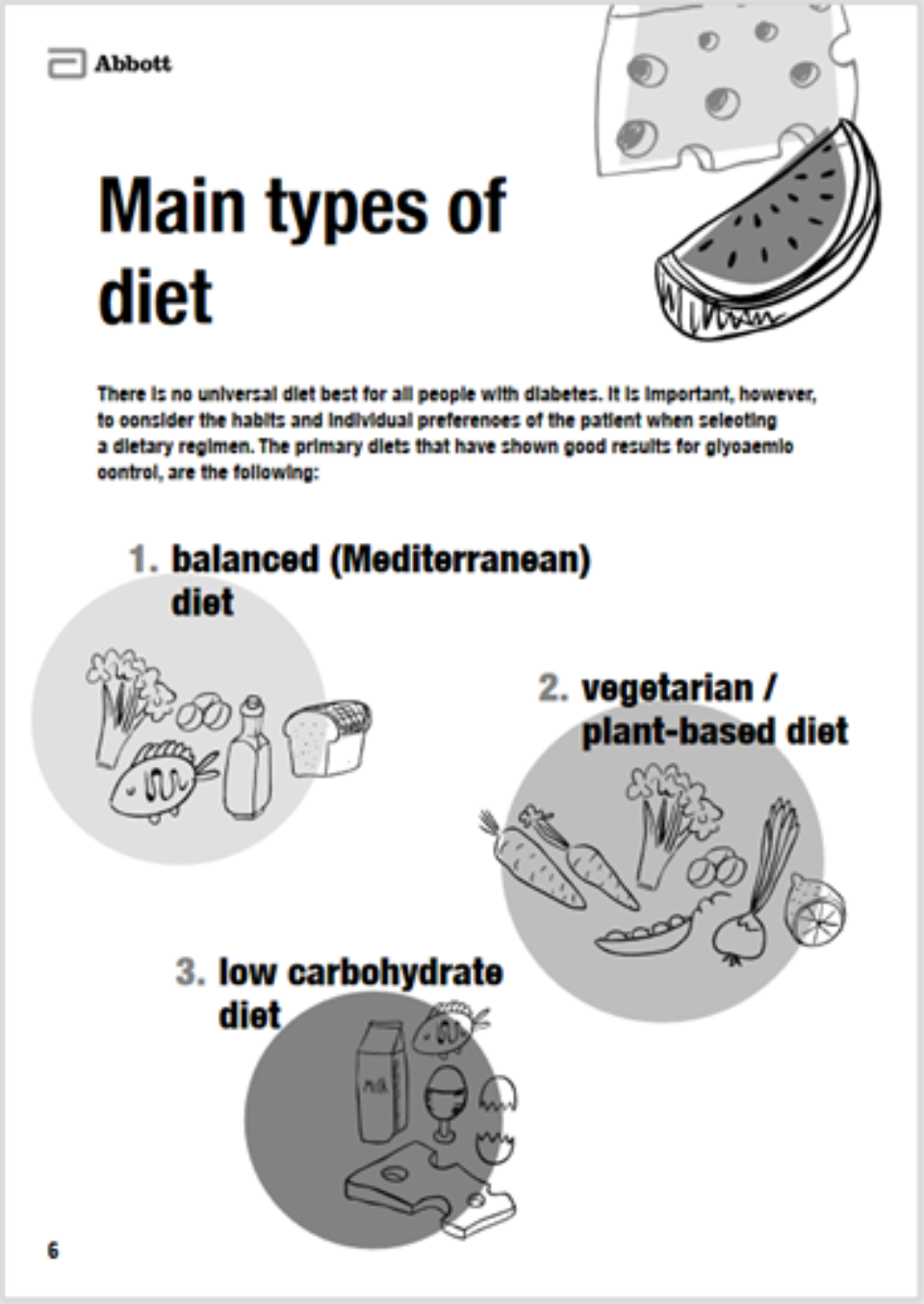
The recently published Abbott e-book suggests once the target weight and glycaemic control is achieved, reversal/remission of Type 2 diabetes can be maintained by adopting either a Mediterranean diet, a Vegetarian/plant-based diet, or a Low Carbohydrate diet, with or without intermittent fasting.
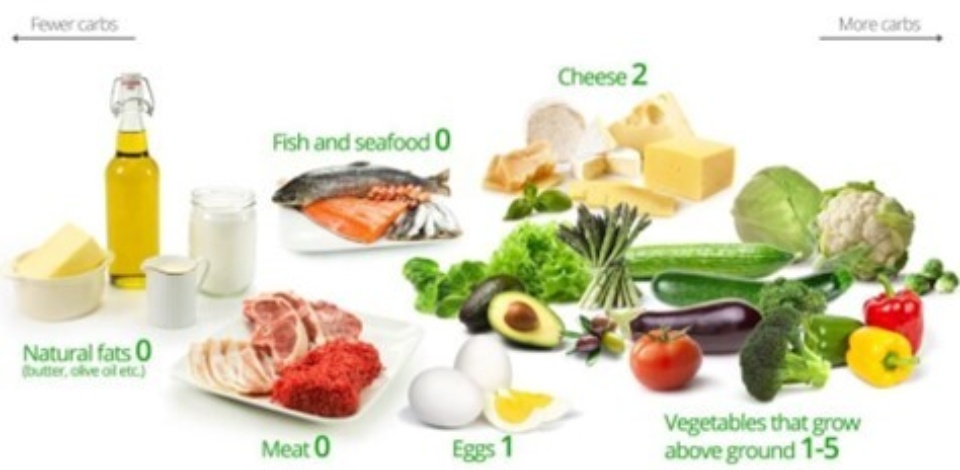
The team at Diet Doctor showcases a Low Carbohydrate/Ketogenic diet, otherwise known as a 'Whole Food Plant-based' (WFPD) diet. Image C/O www.dietdoctor.com
In Conclusion
The American College of Lifestyle Medicine has a seemingly endless benevolent agenda that wards off criticism. However, there is a distinct lack of transparency and full disclosure and a perceived conflict of interest around their promotion of plant-based diets for; - Type 2 Diabetes, heart disease, environmental issues, and their collaboration with Exercise is Medicine.
The authors and facilitators are not only biased against Low Carbohydrate diets but, even more concerningly, biased toward the exclusion of animal proteins and fats, which stem from a devout Religious Ideology.
In America and elsewhere around the world, Lifestyle Medicine has become a movement founded on the Health Reform principles of the Seventh-day Adventist Church, given to their Prophetess in Vision in 1863. Principles which state; - the Garden of Eden diet (fruit, nuts, and seeds) is the God-appointed diet for man and a devout belief that flesh-meat defiles the body, physically, morally, and spiritually.
I am not challenging Seventh-day Adventist beliefs per sae. I am challenging their influence on our health and dietary guidelines, their commercial interests that remain tax-free, and the support/protection they receive from Dietitian and other Health Associations that fiercely protect their 'Plant-based' ideology.
I am challenging their influence on health professionals who are unwittingly becoming medical evangelists for the Seventh-day Adventist Church…
Rhys Southan, an ex-vegan who has researched and extensively referenced the influence of the Seventh-day Adventist Church on the American Dietary Guidelines concludes; - “If the authors of a paper stating that veganism is healthy is because they want more people to be vegan for the animals or the environment, or because they believe God told the founder of their Church, in vision, that fruit, nuts and seeds are the God-Appointed diet for man - why not list this as a possible conflict of interest?”
An inclusive 'Bill of Rights' MUST offer all dietary options regardless of personal or religious bias.
As Dr Gary Fettke says; - encouraging 'fresh, local, and seasonal whole foods based on an individual's environment, and supportive of cultural diversity and food preferences, avoiding added sugars and processed foods' will help ensure optimal protein and fat intake with the accompanying essential vitamins and minerals.
Encouraging fresh, local, and seasonal whole foods based on an individual's environment, and supportive of cultural diversity and food preferences, avoiding added sugars and processed foods
Over-arching recommendations to reduce or eliminate nutrient-poor and hyper-palatable processed foods should complement individualised recommendations, thereby offering the best health outcomes possible, including the remission/reversal of Type 2 diabetes.
There is no 'one-size-fits-all'.
Disclaimer; - I am not anti-religion nor am I anti-vegan. I respect each and every individual’s right to their beliefs and their dietary choices. My concern is; - the right to be given accurate, complete and unbiased information is being taken away from people who choose to include meat, eggs, and dairy in their diet - for their health - by the Vested Interests and Religious Ideology shaping our ‘plant-biased’ dietary and health guidelines.
Written by
